CTOs fear re-architecting 12 months later. Here’s how to avoid that nightmare.
Your telehealth MVP just landed its first enterprise contract. Five pilot clinics become fifty. Then two hundred. Somewhere between clinic 30 and clinic 75, everything starts breaking. Patient intake forms time out. Video sessions drop randomly. The database maxes out connections at 2 PM every Tuesday. Your engineering team stops building features and starts firefighting.
This moment arrives for nearly every successful telehealth startup. The infrastructure that validated your concept cannot support your growth. But here’s the brutal reality: most founders don’t recognize architectural debt until it’s catastrophically expensive to fix. They built an MVP optimized for speed-to-market. They’re now running production workloads on MVP architecture.
The difference between platforms that scale gracefully and those that collapse isn’t luck. It’s architectural decisions made in the first six months of development — decisions that seem inconsequential when you’re serving five clinics but become existential when you’re serving two hundred.
The MVP-to-Production Chasm: Why Good Code Suddenly Fails
MVPs optimize for one thing: proving product-market fit as cheaply as possible. This is correct. But the technical shortcuts that enable rapid validation create technical debt that compounds exponentially under load. What works perfectly for 500 patients per month implodes at 5,000.
The Classic Collapse Pattern
Here’s how the collapse typically unfolds:
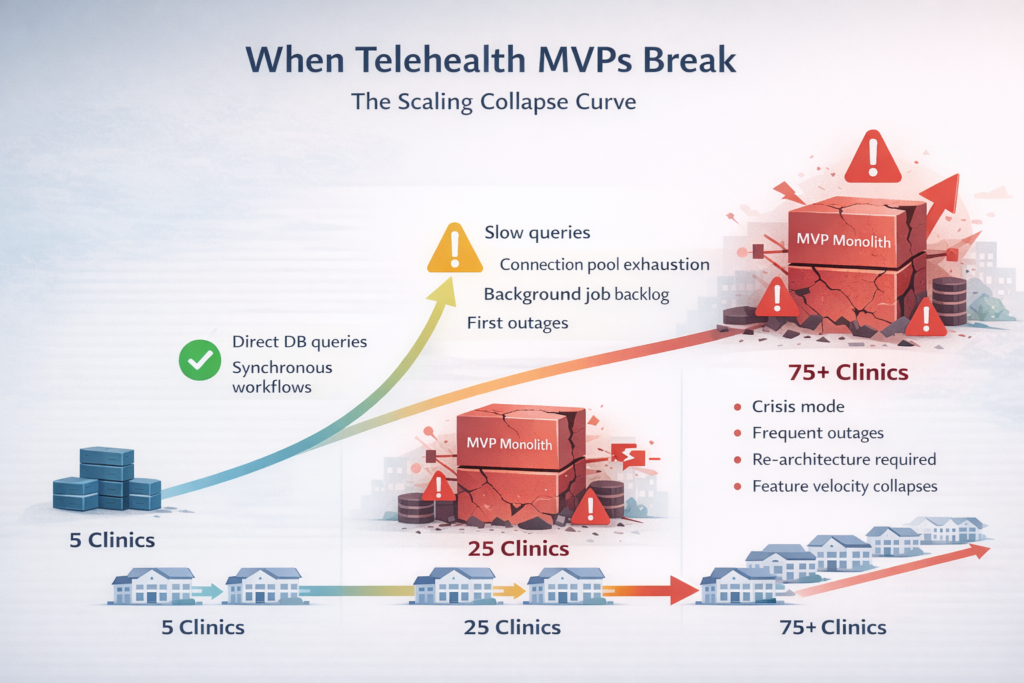
- Months 0-6: MVP development. Single monolithic application. Direct database queries. Synchronous processing. Everything works because scale is trivial. Five clinics, 20 providers, 500 patients. Any decent developer can make this work.
- Months 6-12: Initial traction. Sign 20 more clinics. Traffic grows 10x. First performance issues appear. Database queries slow down. Background jobs pile up. Team adds caching, optimizes queries, and increases server size. Problems are temporarily resolved.
- Months 12-18: Accelerating growth. 50 clinics, 200 providers, 10,000 patients. The architecture can’t absorb this scale. Database connection pool exhaustion becomes routine. Processing backlogs grows faster than they clear. Outages start affecting customer retention.
- Months 18-24: The crisis point. Engineering velocity collapses. Every feature triggers cascading failures. Customer acquisition stalls because demos break. The CTO realizes the platform needs fundamental re-architecture. Estimated timeline: 6-9 months. Cost: 40-60% of engineering capacity.
This pattern repeats across industries, but healthcare technology faces unique pressures. You cannot take the platform offline for re-architecture. You cannot lose patient data during migration. You cannot violate HIPAA during the transition. The re-architecture must happen while continuing to serve production traffic, meet compliance requirements, and ship features that keep customers from churning.
Bad Early Decisions That Haunt Production Systems
Certain architectural choices seem reasonable during MVP development, but create compounding problems at scale. These aren’t obviously terrible decisions. They’re subtle tradeoffs that optimize for short-term velocity at the cost of long-term scalability.
The WordPress Patient Intake Trap
Many telehealth startups build their initial patient intake forms using WordPress, Webflow, or similar content management systems. The reasoning seems sound: why build custom forms when dozens of tools handle this perfectly? You need to validate demand, not optimize infrastructure.
But here’s what this decision actually creates:
- Data Synchronization Nightmare: Patient data starts in WordPress, gets transferred to your core application, then syncs to your EHR integration. Each transfer point risks data corruption, introduces latency, and creates compliance exposure. When intake volume increases 50x, these sync jobs become bottlenecks.
- PHI Sprawl: Protected health information now lives in three separate systems with different security controls. Your HIPAA audit trail fragments across platforms. When breaches occur, you cannot easily determine which systems were compromised or what data was exposed.
- Validation Drift: WordPress validates intake forms differently than your application validates data. Edge cases that WordPress accepts create database corruption in your core system. You discover these mismatches during production outages, not during testing.
- Vendor Lock-In: Replacing WordPress means rebuilding intake forms and migrating historical data. But the forms have evolved over 18 months and accumulated dozens of customizations. Full replacement requires 3-4 months of development while continuing to support the legacy system.
The alternative: Build intake forms as part of your core application from day one. Use form libraries that give you WordPress-level flexibility without introducing external dependencies. Accept that initial development takes two weeks longer. Gain the ability to scale intake processing independently and maintain unified security controls.
Email-Based PHI Transmission
Early-stage telehealth platforms often use email for clinical workflows. Providers receive appointment notifications via email. Lab results get sent as PDF attachments. Patient questions arrive in providers’ inboxes. This seems practical — everyone knows how to use email.
The problems compound as the scale increases:
- Compliance Catastrophe: Email is not HIPAA-compliant by default. Even encrypted email services introduce risks. Providers forward messages to personal accounts. Attachments get saved to unsecured devices. You have no audit trail of who accessed PHI or when. OCR investigators love email-based PHI breaches because they’re indefensible.
- Unscalable Workflow Coordination: At 5 clinics, email-based coordination works. At 50 clinics, provider inboxes receive hundreds of automated messages daily. Critical clinical alerts get buried in notification spam. Providers miss time-sensitive communications because email doesn’t support priority routing or intelligent filtering.
- State Fragmentation: Email becomes the system of record for clinical decisions made outside your application. When you need to reconstruct patient care history, half the data lives in email threads. You cannot query it, report on it, or include it in analytics. Critical business intelligence disappears into email archives.
- Integration Impossibility: Modern healthcare requires API integration with labs, pharmacies, and EHR systems. These integrations cannot interact with email-based workflows. You end up maintaining dual workflows — one email-based for legacy processes, one API-based for new integrations. The integration burden doubles.
The alternative: Build in-application notification and messaging from the start. Use email only as a transport mechanism that links back to your application. All clinical data stays within your security boundary. Providers see unified dashboards instead of fragmented inboxes. You maintain complete audit trails and enable sophisticated workflow automation.
Monolithic Architecture Without Service Boundaries
The MVP launches as a single application. Patient scheduling, video consultations, billing, prescriptions, lab integrations — everything lives in one codebase deployed as one service. This is actually reasonable for MVPs. Microservices introduce complexity that makes no sense at a small scale.
The problem emerges when you need to scale different components independently:
- Resource Contention: Video processing consumes massive CPU and bandwidth. Billing calculations are CPU-light but database-heavy. Lab result parsing is bursty and unpredictable. In a monolith, these workloads compete for the same resources. You cannot optimize infrastructure for each workload independently. You scale everything or nothing.
- Deployment Coupling: Bug fix in the billing module requires deploying the entire application. This redeploys video streaming, patient scheduling, and every other subsystem. Small changes trigger large deployment risks. Teams become paralyzed by fear of breaking unrelated features.
- Team Coordination Overhead: As engineering headcount grows, everyone works in the same codebase. Merge conflicts become daily occurrences. Code reviews bottleneck on senior engineers who understand the full system. Parallelizing development becomes impossible because changes in one module break assumptions in others.
- Cascade Failures: Bug in lab result parsing crashes the entire application. Billing calculation error takes down patient scheduling. Memory leak in video streaming affects prescription processing. No isolation means every failure is a total failure.
The alternative: Start with a modular monolith that enforces clear boundaries between domains. Patient scheduling, clinical workflows, billing, and integrations live in separate modules with defined interfaces. When scale demands it, extract modules into independent services. The refactoring effort drops from 6 months to 2 weeks because boundaries already exist.
Why Event-Driven Architecture Becomes Non-Negotiable at Scale
Most telehealth MVPs use synchronous request-response patterns for everything. The user submits a form, the application processes it immediately, and returns a response. This works until processing time exceeds acceptable latency or concurrent requests exceed available resources.
The Synchronous Processing Death Spiral
Consider a typical patient appointment flow in a synchronous architecture:
- Patient books an appointment through the web interface
- Application checks provider availability in the database
- Creates an appointment record
- Sends confirmation email to patient
- Sends notification to the provider
- Updates calendar in external EHR via API
- Triggers an insurance verification check
- Returns a confirmation page to the patient
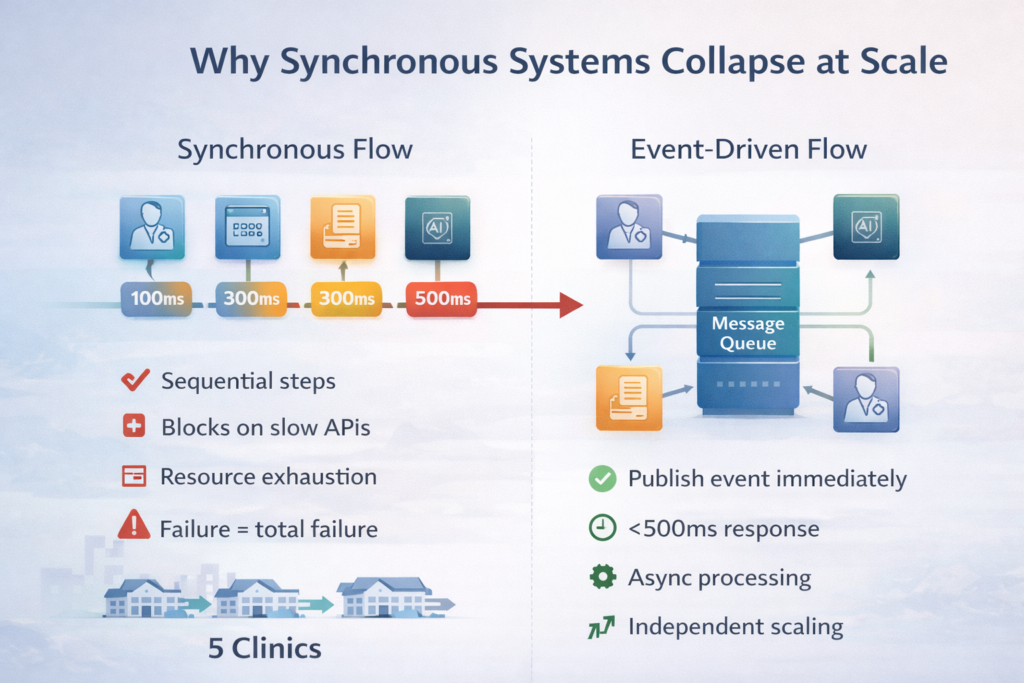
All eight steps happen sequentially during the patient’s page load. If the EHR API is slow, the patient waits. If insurance verification times out, the appointment booking fails. If email sending blocks, everything blocks. The entire user experience couples to the slowest dependency.
At scale, this creates devastating problems:
- Latency Multiplication: Each step adds 100-500ms of latency. Eight steps = 2-4 seconds minimum response time. Users perceive anything over 1 second as slow. Appointment booking becomes frustratingly sluggish, reducing conversion rates.
- Failure Amplification: If step 6 fails, steps 7 and 8 never execute. Patient receives confirmation, but insurance doesn’t get verified. Provider gets notified, but EHR never updates. Data consistency becomes impossible to maintain across all dependent systems.
- Resource Exhaustion: Each booking request holds a database connection, web server thread, and memory for 2-4 seconds. At 50 concurrent bookings, you need 50 database connections. At 500 concurrent bookings, you’ve exceeded your connection pool and the new requests queue indefinitely.
- Retry Chaos: When external APIs timeout, your application retries. But the patient also hits refresh. Now you have duplicate appointment bookings, duplicate emails, and duplicate EHR updates. Deduplication becomes a nightmare.
Event-Driven Architecture as the Solution
Refactor the same appointment flow with event-driven architecture:
- Patient submits appointment booking request
- Application validates availability and creates appointment record (200ms)
- Publishes ‘AppointmentBooked’ event to the message queue
- Returns a confirmation page to the patient immediately
Background workers asynchronously process the event:
- Email service consumes the event, sends confirmation emails
- EHR integration service consumes events, updates the external calendar
- Insurance verification service consumes the event, checks coverage
- Analytics service consumes events, updates dashboards
The benefits compound:
- Predictable Latency: User experience depends only on critical path operations. Response times stay under 500ms regardless of downstream complexity. Patient satisfaction increases because the interface feels fast.
- Graceful Degradation: If EHR integration is down, appointments still be booked successfully. The EHR update queues for retry when the service recovers. Users never experience total failures, only delayed processing of non-critical operations.
- Independent Scaling: Email sending spikes during business hours. Add more email workers. Insurance verification is CPU-intensive. Scale that service independently. Each component optimizes for its specific workload characteristics.
- Automatic Retry and Idempotency: Message queues handle retries automatically. Services become idempotent — processing the same event twice produces the same result. Duplicate bookings become impossible through design, not complex deduplication logic.
The transition from synchronous to event-driven architecture is the most important architectural evolution during scaling. Platforms that defer this transition find themselves rewriting increasingly complex synchronous code to handle concurrency, failures, and latency. Platforms that adopt event-driven patterns early gain scalability as an emergent property of their architecture.
AI System Isolation: Why Tightly Coupled AI Destroys Reliability
AI features have become table stakes in telehealth platforms. Automated triage, clinical decision support, documentation generation, diagnostic assistance — these capabilities differentiate modern platforms from legacy systems. But integrating AI directly into core application logic creates cascading reliability problems.
The Tightly Coupled AI Disaster Pattern
Early-stage platforms typically implement AI features like this:
- Patient submits symptoms through the intake form
- Application calls the OpenAI API directly during request processing
- AI generates a triage recommendation
- The application displays a recommendation to the patient
This creates multiple failure modes that compromise the entire platform:
- Latency Unpredictability: AI API calls take 2-30 seconds, depending on model complexity and API queue depth. Core user workflows that should complete in milliseconds now take seconds. Users cannot distinguish between ‘AI is processing’ and ‘application is broken.’ Perceived reliability collapses.
- Cascade Failures: OpenAI rate-limits your API key during high traffic. Now your entire patient intake system fails. A third-party AI service outage becomes a total platform outage. Your SLA depends on external services you cannot control.
- Resource Starvation: AI API calls hold database connections and web server threads while waiting for responses. At scale, AI processing consumes all available resources. Non-AI features like appointment scheduling start failing because AI features monopolize connection pools.
- Compliance Complexity: PHI sent to AI services requires Business Associate Agreements. But if AI is deeply integrated, you cannot easily switch providers or run models on-premises. Compliance requirements force expensive architectural changes.
- Testing Nightmare: Automated tests that call real AI APIs are slow and expensive. Mocking AI responses is complex and brittle. Your test suite either takes 45 minutes to run or provides inadequate coverage. Engineering velocity suffers.
Architectural Isolation for AI Systems
Production-grade AI integration requires strict isolation:
- Dedicated AI Service Layer: AI operations live in separate services with their own resource pools. Core application publishes events requesting AI analysis. AI service processes asynchronously and publishes results. If the AI service crashes, the core platform continues functioning.
- Fallback Strategies: Application defines acceptable behavior when AI is unavailable. Manual triage workflows activate automatically. Users experience degraded functionality, not total failure. Business continuity doesn’t depend on AI availability.
- Circuit Breakers: When AI API error rates exceed thresholds, circuit breakers open automatically. The system stops making failing API calls that waste resources. Manual intervention resets circuits after confirming service recovery.
- Result Caching: Common AI queries get cached aggressively. ‘Headache and fever’ triage runs once; the result serves thousands of patients. Cache invalidation handles model updates. Response times drop from seconds to milliseconds for cached results.
- Provider Abstraction: The AI service interface abstracts specific providers. Switching from OpenAI to Anthropic or deploying on-premises models requires changing one service, not refactoring the entire application. Compliance requirements drive provider selection without forcing re-architecture.
The cost of AI isolation feels high during MVP development. Building abstraction layers and async processing adds complexity. But this investment pays compounding returns. When you need to migrate to different AI providers for cost or compliance reasons, the change takes days instead of months. When AI services experience outages — and they will — your platform remains operational.
From 5 Clinics to 200: The Scaling Journey in Practice
Understanding how different architectures perform at specific scale points helps anticipate problems before they become crises. Here’s what the scaling journey looks like with realistic metrics and failure modes:
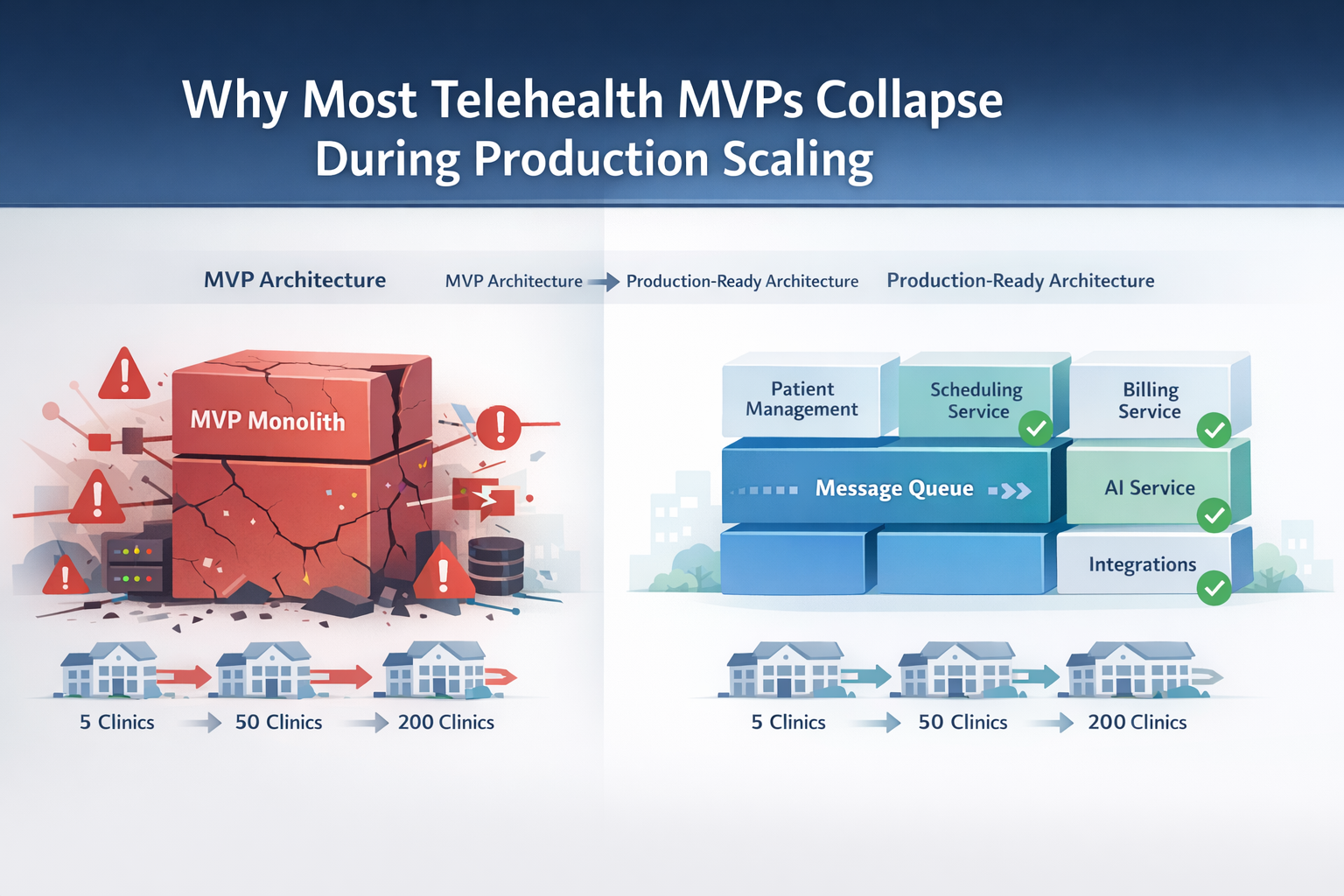
| Scale | Characteristics | MVP Architecture Issues | Production-Ready Architecture |
| 5-10 Clinics~500 patients/month | Single geographic regionBasic feature set1-2 concurrent providers onlinePredictable usage patterns | Everything worksNo performance issuesTechnical debt invisibleManual operations acceptable | Minor over-engineeringExtra complexity without clear benefitHigher development costSlower initial delivery |
| 25-50 Clinics~5,000 patients/month | Multi-state operationSpecialty services launching10-20 concurrent providersUsage spikes during business hours | Database query slowdownsPeriodic connection pool exhaustionBackground job backlogsFirst production incidentsCaching band-aids applied | Smooth operationPredictable performanceNo manual intervention requiredReliable monitoring and alertingEngineering team builds features |
| 75-125 Clinics~15,000 patients/month | National footprintComplex feature requirements40-75 concurrent providersDistributed team managing platform | Crisis mode beginsFrequent outagesCustomer escalationsEngineering firefighting6-month re-architecture plannedFeature velocity collapses | Some optimization neededIndividual service scalingMinor architectural adjustmentsMaintained engineering velocityProactive capacity planning |
| 150-200 Clinics~30,000 patients/month | Enterprise contractsCompliance requirements100+ concurrent providers24/7 operation expectations | Total re-architecture requiredPlatform barely functionalCustomer retention threatenedEngineering team demoralizedFounder regret intensifies | Scaling individual componentsCost optimization focusAdvanced observabilityPredictable operationsCompetitive advantage established |
The gap between ‘MVP architecture issues’ and ‘production-ready architecture’ represents the difference between platforms that scale gracefully and those that require emergency re-engineering. Notice that production-ready architecture faces challenges at each scale point — but these are optimization challenges, not existential crises.
The Critical Inflection Points
Two inflection points determine whether platforms survive the scaling journey:
- The 25-Clinic Inflection (MVP Architecture): This is where technical shortcuts start causing visible problems. Database queries that completed in 50ms now take 2 seconds. Background jobs that used to be processed in minutes now take hours. If you don’t recognize these symptoms as architectural problems — not just optimization opportunities — you’ll apply increasingly desperate band-aids while the fundamental issues compound.
- The 75-Clinic Inflection (Emergency Re-Architecture): This is the point of no return. Band-aids stop working. You need fundamental architectural changes while serving production traffic. Every day you delay costs exponentially more. Customer acquisition stalls because demos break. Retention suffers because reliability collapses. The window to fix this gracefully has closed.
Platforms with production-ready architecture from the start avoid both inflection points entirely. They encounter optimization challenges but never face existential architectural crises. This is why architectural decisions made during the first six months of development determine the next three years of engineering productivity.
Architecting for Phase 2 from Day One
The optimal strategy isn’t building microservices and event-driven architecture from the first line of code. That introduces premature complexity that slows validation. But it also isn’t building the simplest possible MVP and hoping you’ll have time to re-architect later. That creates technical debt that becomes unpayable.
The middle path: build a modular monolith with clear boundaries that can evolve into distributed services when scale demands it.
The Modular Monolith Pattern
Start with these architectural principles:
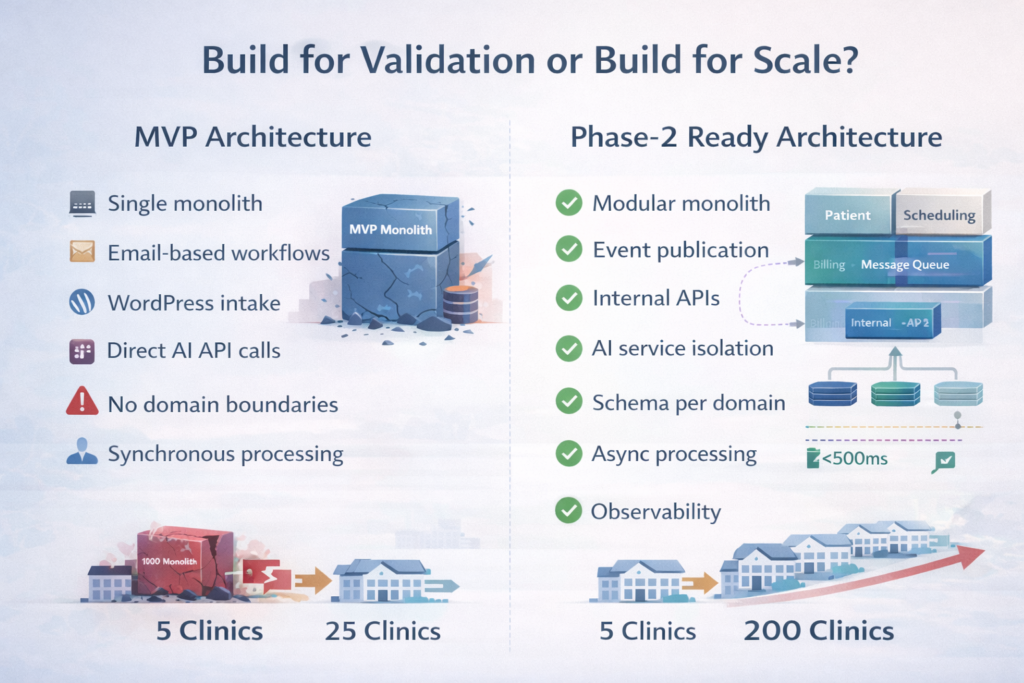
- Domain-Driven Boundaries: Organize code around business domains (patient management, scheduling, clinical workflows, billing), not technical layers (controllers, models, views). Each domain owns its data and exposes well-defined interfaces. Dependencies flow in one direction.
- Database Schemas Per Domain: Even in a single database, use separate schemas for each domain. Patient data lives in patient_schema. Billing data lives in billing_schema. Domains never directly query another domain’s schema. This enforces boundaries that enable later database separation.
- Internal APIs: Domains communicate through defined interfaces, not direct method calls. When scheduling needs patient data, it calls the patient domain’s API. These internal APIs look like HTTP APIs but execute in-process initially. Later, they become actual HTTP APIs without changing the calling code.
- Event Publication: Domains publish events for significant state changes. Initially, these events trigger in-process handlers. As the scale grows, migrate to external message queues without changing event publishers. Event-driven architecture becomes a configuration change, not a rewrite.
- Separated Build Artifacts: Structure build system to produce separate artifacts per domain, even if deployed together initially. Testing, deployment, and monitoring treat each domain semi-independently. This reveals coupling problems early and makes extraction straightforward.
This pattern delivers 80% of microservices’ scalability benefits with 20% of the complexity cost. You deploy a single application that’s easier to debug and monitor. But the architecture supports the extraction of domains into independent services when specific scaling pressures emerge.
The Migration Path to Production Architecture
Here’s how modular monoliths evolve into distributed systems:
- Identify Scaling Bottleneck: Monitoring reveals which domain creates resource pressure. Video processing consumes excessive CPU. Lab integration generates database connection spikes. Focus extraction on the component that’s actually causing problems, not the one that feels architecturally important.
- Extract Domain to Service: Deploy the domain code as an independent service. Change internal API calls to HTTP. Migrate from in-process events to a message queue. Use feature flags to control which implementation runs. This enables incremental migration and instant rollback if problems emerge.
- Separate Data Stores: Migrate the domain’s database schema to a dedicated database. Use replication and dual-writes during the transition to ensure consistency. Validate data in parallel before cutting over completely. The schema separation you implemented initially makes this mechanical, not creative.
- Scale Independently: Now the extracted service scales based on its specific workload. Add compute for video processing. Add memory for caching. Add database replicas for read-heavy operations. Optimization targets specific bottlenecks instead of guessing across the entire monolith.
- Repeat for Next Bottleneck: Don’t extract everything at once. Extract only what scaling pressures demand. Most domains stay in the monolith indefinitely. You end up with 3-5 extracted services and a lean monolith, not 47 microservices that nobody can reason about.
This migration path turns re-architecture from a 6-month development freeze into a series of 2-week incremental improvements. Teams maintain feature velocity while progressively addressing scaling bottlenecks. The technical risk of migration drops dramatically because changes happen incrementally with validation at each step.
The Phase 2-Ready Architecture Checklist
Before writing the first line of code, ensure your architecture includes:
- Domain Boundaries: Clear separation between patient management, clinical workflows, scheduling, billing, and integrations with no cross-domain database queries
- Event Publication: All state changes publish events even if initially handled in-process, with event schema versioning from day one
- Asynchronous Processing: Background job infrastructure for any operation that doesn’t require immediate user feedback, with retry logic and idempotency
- Database Connection Pooling: Properly sized connection pools with monitoring alerts before exhaustion, separate pools for transactional and analytical workloads
- Caching Strategy: Multi-layer caching with cache invalidation patterns defined, not bolted on when performance degrades
- Observability: Structured logging, distributed tracing, and metrics from the start with defined SLOs for critical user journeys
- Feature Flags: A toggle system for gradually rolling out changes and instantly disabling problematic features without deployments
- API Versioning: Version all APIs, including internal ones, with deprecation policies and migration paths planned before shipping v1
- Database Migration Strategy: Automated schema migrations that can roll forward and backward, tested in staging before production deployment
- Integration Abstractions: Third-party services accessed through internal interfaces, not direct dependencies scattered throughout code
These patterns add approximately 15-20% to initial development time. But they eliminate 6-12 months of re-architecture work and the associated opportunity cost of halted feature development. The ROI on this investment typically exceeds 500% by month 18.
The Real Cost of Getting It Wrong
Let’s quantify what ‘collapsing during production scaling’ actually costs in concrete terms:
Engineering Capacity
- Emergency Re-Architecture: 6-9 months of 60-80% engineering team capacity. On a 10-person engineering team, that’s 60-90 engineer-months of work that produces zero new features for customers.
- Opportunity Cost: Features that would have driven expansion revenue don’t get built. Competitive advantages evaporate as rivals ship capabilities you can’t support. Revenue growth stalls while engineering rebuilds infrastructure.
- Team Morale: Engineers signed up to build healthcare technology, not rewrite code they shipped 18 months ago. Attrition increases. Recruiting suffers when word spreads that your platform is ‘in crisis mode.’ Rebuilding the team takes 6-12 months after the technical rebuild completes.
Customer Impact
- Reliability Issues: Production outages during the collapse phase drive customer churn. Healthcare providers cannot tolerate unreliable platforms. Each outage gives customers justification to evaluate alternatives.
- Sales Cycles: Enterprise prospects conduct technical due diligence. When they discover architectural problems, deals stall or die. Rebuilding trust takes longer than rebuilding architecture.
- Feature Stagnation: Nine months without meaningful feature releases means customers questioning whether to renew. Competitors advertise capabilities you promised but couldn’t deliver because engineering was rebuilding infrastructure.
Financial Impact
- Infrastructure Costs: Poorly architected systems require 3-5x the infrastructure of well-designed systems to deliver the same performance. You’re overpaying for AWS while delivering a worse user experience.
- Customer Acquisition Cost: Longer sales cycles and higher churn rates increase CAC by 40-70%. Your unit economics deteriorate at exactly the moment when you need to demonstrate scalable growth to investors.
- Fundraising Challenges: Sophisticated investors recognize architectural crisis during due diligence. Valuations suffer. Terms worsen. Some rounds fail entirely because investors don’t believe you can fix the platform while maintaining growth.
Conservative estimate: architectural collapse costs 12-18 months of progress and 2-3x the engineering investment compared to building scalable architecture initially. Aggressive estimate: it kills the company through lost competitive position and inability to serve the market you created.
Conclusion: Architecture as Strategic Advantage
The decision point arrives during the first design conversation, not during the scaling crisis. You either build modular architecture with domain boundaries, event-driven patterns, and separated concerns — or you build MVP code that optimizes for immediate validation at the cost of future scalability.
Neither choice is objectively wrong. If your goal is to validate product-market fit with minimal investment, accepting technical debt makes sense. But understand the debt compounds exponentially. The cost to fix it grows faster than revenue. By the time you need a scalable architecture, the window to build it gracefully has closed.
Founders transitioning from MVP to serious SaaS face this reality: you cannot scale systems that weren’t designed to scale. You can only replace them. The question becomes whether you replace them proactively during controlled migration or reactively during crisis mode when customers are churning, and competitors are gaining ground.
Production-ready architecture from day one costs 15-20% more initially but delivers compounding returns. You scale from 5 clinics to 200 by adding infrastructure, not rewriting code. Engineering teams maintain velocity through growth phases instead of halting feature development for emergency re-architecture. Reliability becomes a competitive advantage instead of an existential threat.
Partner with Trembit for Scalable Architecture
Trembit specializes in building telehealth platforms that scale from MVP to enterprise without catastrophic re-architecture. Our system architects understand the difference between code that validates product-market fit and infrastructure that supports production growth.
We implement modular monolith patterns that evolve gracefully into distributed systems. We build event-driven architectures that handle spike loads without resource exhaustion. We isolate AI systems so experimental features don’t compromise core platform reliability. We establish domain boundaries that enable independent team velocity as your engineering organization grows.
When you’re ready to build a telehealth platform that scales from 5 clinics to 200 without emergency re-architecture, we bring the expertise and engineering discipline to make it happen. We’ve navigated this transition dozens of times. We know which architectural decisions compound value and which create technical debt. Most importantly, we know how to balance rapid market validation with long-term technical sustainability.