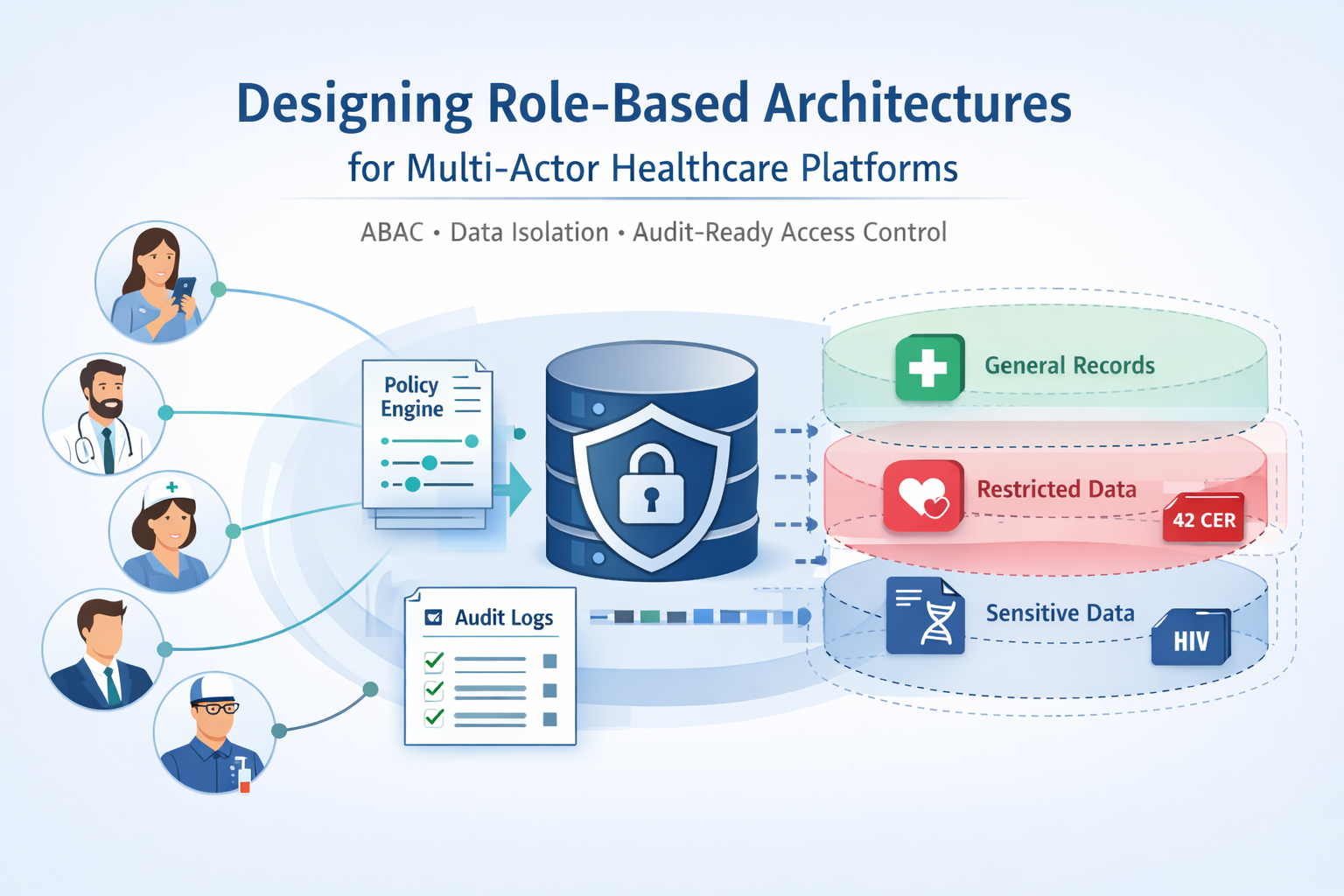
Healthcare platforms operate in a uniquely complex permission landscape. A single patient record might be accessed by the patient themselves, their primary care physician, a consulting specialist, a nurse coordinator, billing staff, quality assurance reviewers, external lab technicians, insurance verifiers, and platform administrators — each with legitimate but dramatically different access needs. Traditional role-based access control fails catastrophically in this environment because it cannot capture the nuanced, contextual, and relationship-dependent nature of healthcare data access.
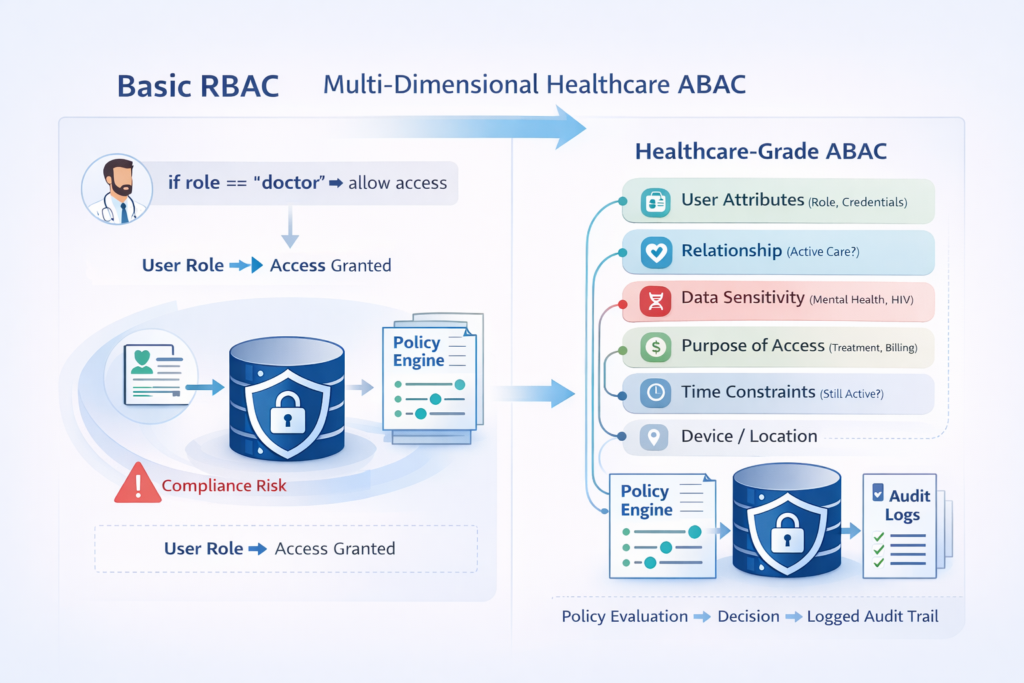
The gap between “we implemented RBAC” and “our access control withstands regulatory scrutiny” is vast. Most platforms implement crude role checking — if the user. role == “doctor” then grants access — and discovers during their first compliance audit that this approach creates both security vulnerabilities and HIPAA violations. Healthcare RBAC requires architectural sophistication that goes far beyond checking user roles at the application boundary.
The Multi-Actor Permission Matrix: Beyond Simple Roles
Healthcare platforms serve fundamentally different user types with conflicting access requirements. Understanding these actors and their permission needs drives architectural decisions throughout the entire system.
The Four Core Actor Categories
Patients: Data Subjects with Limited Scope
Patients access only their own data, but they need comprehensive visibility into everything related to their care. They view appointments, lab results, prescriptions, billing statements, and clinical notes. However, they cannot access the underlying clinical workflows, provider scheduling systems, or administrative operations. Their access is deeply personalized but narrowly scoped.
The architectural challenge: patients expect instant access to new information (lab results posted, prescription filled, appointment scheduled) without manual permission grants. The system must automatically establish access rights when new data entities are created and link them to the correct patient. Failure creates support burdens (“Why can’t I see my test results?”) and compliance risks (showing the wrong patient’s data).
Clinicians: Relationship-Based Access with Clinical Context
Physicians, nurses, and allied health professionals require access based on active care relationships. A cardiologist treating a patient needs full access to that patient’s cardiac history, medications, and recent vitals. But they don’t need access to the patient’s dermatology records from five years ago or their current mental health treatment with a different provider. Access derives from documented clinical relationships, not blanket permissions.
The architectural challenge: clinical relationships are temporal and context-dependent. A consulting physician needs access during the consultation period, then loses access when the consultation ends. Emergency room physicians need immediate access to any patient who presents, with retroactive justification. The system must grant appropriate access in real-time based on clinical workflows, not pre-configured permission lists.
Administrators: Broad Access with Audit Requirements
Billing specialists, quality reviewers, compliance officers, and technical support staff need access patterns that cross patient and provider boundaries. They analyze aggregate data, investigate billing discrepancies, respond to patient complaints, and troubleshoot technical issues. Their access requirements are broader but less clinically focused.
The architectural challenge: administrative access creates the highest compliance risk. These users can access large volumes of PHI without direct clinical justification. Every access must be logged, justified, and auditable. The system must enforce least privilege while enabling legitimate operational needs. Break-glass procedures for urgent access require immediate alerting and post-access review.
Partner Entities: External Access with Limited Scope
Labs, pharmacies, imaging centers, insurance verifiers, and third-party EHR systems access specific data subsets through defined interfaces. They need real-time access to order information, results transmission capabilities, and verification data. But they should never see patient data beyond their specific operational scope.
The architectural challenge: partner access happens through APIs, not user interfaces. Rate limiting, authentication, and authorization must work at API request granularity. A lab partner should access only orders sent to their facility, not all platform lab orders. The system must enforce data isolation at the organizational boundary while maintaining integration performance.
Permission Dimensions Beyond Role
Traditional RBAC assigns permissions based solely on user role. Healthcare platforms require multi-dimensional authorization that considers:
Relationship Context
- Is this provider currently treating this patient?
- Was treatment within the last 6 months (continuity of care)?
- Is this an emergency access situation?
- Did the patient explicitly grant access to this provider?
Data Sensitivity
- Substance abuse treatment records require additional protections (42 CFR Part 2)
- Mental health notes may have restricted access even within care teams.
- HIV status, genetic information, and reproductive health have special handling
- Some jurisdictions require patient consent for certain data categories.
Purpose of Access
- Treatment operations have broader permissions than payment or healthcare operations.
- Research access requires de-identification or explicit consent.
- Quality improvement has different restrictions than routine care.
- Marketing use is prohibited without explicit authorization.
Temporal Constraints
- Emergency access grants immediate permissions with a post-access audit
- Consultation access expires when the consultation period ends.
- Administrative access may be time-limited to specific investigation windows.
- Patient access to certain records may have mandatory waiting periods (psychotherapy notes)
Location and Device Context
- Accessing from the clinic network vs. public WiFi affects available operations
- Managed devices get different permissions than BYOD.
- Geographic restrictions may apply for compliance (data residency)
- Certain operations require multi-factor authentication regardless of role.
This multi-dimensional model cannot be expressed in simple role-permission mappings. It requires architectural support for policy evaluation engines that assess each access request against multiple criteria in real-time.
Architectural Patterns for Healthcare RBAC
Implementing truly robust healthcare access control requires specific architectural patterns that most platforms overlook during initial development.
Attribute-Based Access Control (ABAC) as Foundation
Replace role-based permission checks with attribute-based policy evaluation. Every access request includes:
- User attributes (role, department, provider credentials, employment status)
- Resource attributes (patient identifier, data sensitivity classification, record type)
- Context attributes (purpose of access, location, device security posture, time)
- Relationship attributes (active care relationship, consultation status, delegation chain)
Policies evaluate these attributes to make authorization decisions:
PERMIT access to clinical_note IF:
– user.role IN [‘physician’, ‘nurse’] AND
– active_care_relationship(user, resource.patient) AND
– resource.sensitivity_level <= user.clearance_level AND
– access.purpose = ‘treatment’ AND
– current_time WITHIN relationship.active_period
This approach handles complex scenarios that break simple RBAC. When a physician views a patient record, the system evaluates whether an active care relationship exists, whether the data sensitivity requires additional clearance, whether the access purpose is documented, and whether temporal constraints are satisfied. All of this happens in milliseconds during the request.
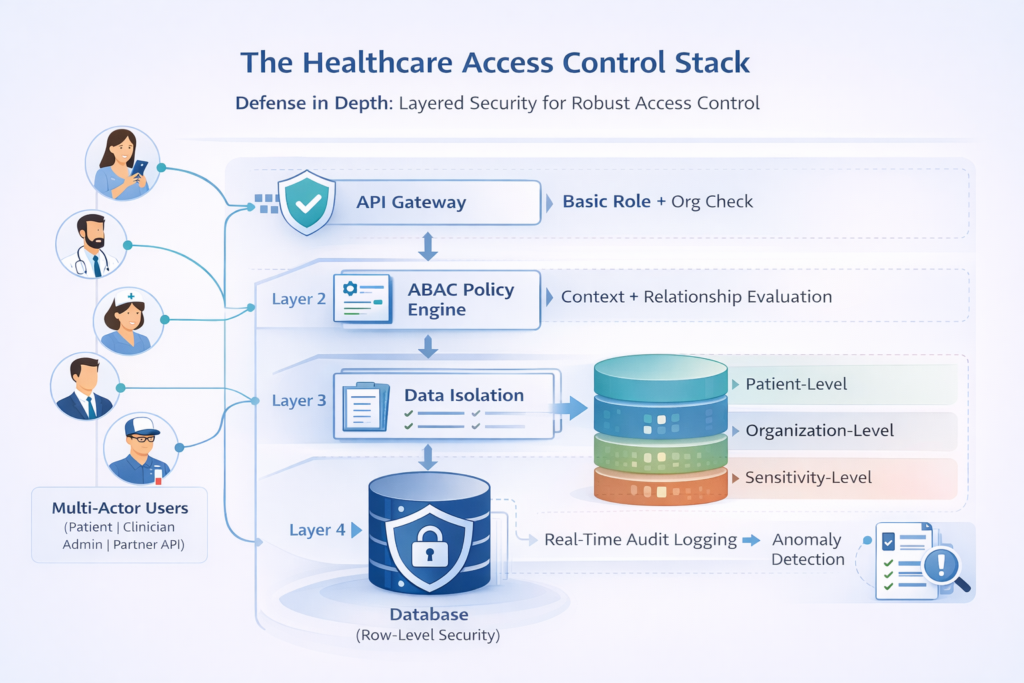
Data Isolation Boundaries
Healthcare platforms must enforce isolation at multiple levels simultaneously:
Patient-Level Isolation
Every data access query includes patient identifier filtering. Database schemas enforce patient_id foreign keys on all PHI-containing tables. Application frameworks automatically inject patient scoping into queries. This prevents accidental cross-patient data leakage from coding errors.
Implementation: Use row-level security in PostgreSQL or similar database-enforced isolation. The database refuses queries that attempt to access patient data without appropriate patient_id filtering, even if the application code has bugs. This creates defense in depth, where authorization failures at the application layer don’t automatically expose other patients’ data.
Organization-Level Isolation
Multi-tenant platforms serving multiple healthcare organizations require strict organizational boundaries. Clinic A’s users cannot access Clinic B’s patient data, operational analytics, or configuration. The system enforces organization_id filtering at the same architectural level as patient_id filtering.
Implementation: Use separate database schemas per organization for the strongest isolation, or implement comprehensive organization_id scoping with database-level enforcement. Consider data residency requirements that may require geographic isolation for certain organizations.
Sensitivity-Level Isolation
Certain data categories require additional access controls beyond standard patient and organization scoping:
| Data Category | Additional Protections |
| Substance Abuse Treatment (42 CFR Part 2) | Separate consent required; cannot be disclosed even for treatment without explicit patient authorization |
| Mental Health Psychotherapy Notes | Accessible only to note author unless explicitly shared; not part of standard medical record |
| Genetic Information | Restrictions on disclosure to insurers and employers; requires specific consent for research |
| HIV/AIDS Status | State-specific restrictions; often requires additional consent for disclosure |
| Reproductive Health | May require additional privacy protections depending on jurisdiction and patient age |
Implementation: Tag sensitive records with classification metadata. Implement separate permission checks for sensitive categories. Audit logs distinguish between standard record access and sensitive category access. Consider physical separation (different database tables) for the highest sensitivity data to prevent accidental exposure through application bugs.
Fine-Grained Permission Layers
Healthcare access control operates at multiple granularity levels:
Field-Level Permissions
Within a single patient record, different fields have different sensitivity and access requirements. A nurse may view vital signs and current medications but not financial information or certain clinical notes. Billing staff access payment details, but not clinical data beyond diagnosis codes needed for claims.
Implementation approaches:
View-Based Filtering: Define database views that expose different field subsets based on user role. Query the appropriate view instead of the base tables. This pushes filtering to the database layer for consistency and performance.
Dynamic Field Redaction: Retrieve full records but redact fields based on user permissions before serialization. This allows flexible permission rules but requires careful implementation to prevent leaking data through error messages or API responses.
Graph-Based Access Control: Model data as a graph where nodes represent data elements and edges represent access permissions. Traverse the graph based on user attributes to determine accessible fields. This supports complex scenarios like “nurses can view medications prescribed by physicians in their department.”
Operation-Level Permissions
Different roles can perform different operations on the same data:
- Patients: Read-only access to their records (in most cases)
- Physicians: Read and create clinical notes; update treatment plans; order tests
- Nurses: Read clinical data; update vitals and care coordination notes
- Billing staff: Read diagnosis codes; update billing records; cannot modify clinical data
- Administrators: Read for support purposes; no modification except under documented break-glass scenarios
Implementation: Separate permissions for create, read, update, delete, and custom operations. Enforce at the API layer before database operations. Log all operations with the user context for audit trails.
Time-Based Permissions
Access rights change based on temporal context:
- Active care relationships grant immediate access.
- Continuity of care may extend access 6-12 months after the last encounter.
- Historical access for treating new conditions related to past treatment
- Emergency access grants temporary elevated permissions with mandatory post-access review
Implementation: Include temporal constraints in authorization policies. Use database triggers to automatically expire access grants. Implement background jobs that review and revoke stale permissions.
Audit Design for Regulatory Compliance
Access control without comprehensive auditing is meaningless. Regulators don’t trust your permission logic—they require proof that it works correctly and evidence when it fails.
What to Log for Every Access
Minimum Logging Requirements:
- User identifier and role at time of access
- Patient identifier or data set accessed
- Specific fields or records viewed
- Timestamp with timezone
- Access purpose (treatment, payment, operations, patient request)
- Source IP address and device identifier
- Access method (UI, API, batch process)
- Authorization decision (granted, denied, why)
- Session identifier for correlation
Enhanced Logging for Sensitive Access:
- Manager/supervisor who must review access
- Documented clinical justification for emergency access
- Patient consent status for restricted categories
- Breakglass override documentation
- Data export or bulk access indicators
- Query parameters that might indicate anomalous access patterns
Audit Log Architecture
Critical Design Principles:
Immutability: Audit logs must be append-only with no deletion capability. Use write-once storage or blockchain-style chaining where each entry includes a hash of the previous entry. This prevents tampering that would invalidate the entire audit trail.
Separation: Audit logs should not share infrastructure with application databases. Log to separate storage systems that application code cannot modify. This prevents compromised application servers from erasing evidence.
Real-Time Streaming: Don’t batch audit logs. Stream them to separate systems in real-time so evidence exists even if the application crashes or gets compromised immediately after access.
Cryptographic Signing: Sign audit entries cryptographically to prove they haven’t been modified. Include timestamps from trusted time sources to prevent backdating.
Retention: HIPAA requires a 6-year retention minimum. Many organizations implement a 7+ years to account for the statute of limitations. Consider regulatory requirements in your jurisdiction.
Automated Anomaly Detection
Static audit logs are necessary but insufficient. Implement automated analysis that alerts on suspicious patterns:
Volume Anomalies:
- User is accessing 10x more records than typical for their role.
- Spike in access to sensitive data categories.
- Bulk exports or unusual query patterns
- Access to patients outside the normal geographic service area
Relationship Anomalies:
- Access without a documented care relationship
- Access to VIP patients by users without a clinical justification
- Access to employees’ or colleagues’ records
- Repeated access denials (possible privilege escalation attempt)
Temporal Anomalies:
- Access outside normal working hours without emergency justification
- Access to records not relevant to current patient encounters
- Continued access after employment termination
- Access to deceased patients without a legitimate administrative reason
Behavioral Anomalies:
- Access patterns inconsistent with the user’s historical behavior
- Navigation patterns that suggest systematic data collection
- Rapid sequential access suggests automated scraping
- Access from unusual locations or devices
These detection systems generate alerts for security teams to investigate. They don’t automatically block access (which could interfere with legitimate care) but ensure rapid response to potential breaches.
Compliance Logging: Evidence That Survives Audits
OCR audits, breach investigations, and compliance certifications require specific evidence that your access control actually works. Generic logging doesn’t meet these requirements.
Demonstrable Compliance Evidence
Access Control Effectiveness:
- Reports showing denied access attempts with justification
- Proof that users can only access data within their assigned scope
- Evidence that permissions follow the least privilege principle
- Documentation of permission review and cleanup processes
Separation of Duties:
- Proof that no single user can create accounts and assign permissions
- Evidence that developers cannot access production PHI
- Audit trails showing multi-party approval for sensitive operations
- Documentation that administrative access requires justification and review
Breach Detection and Response:
- Timestamped alerts on anomalous access patterns
- Evidence of an investigation into security alerts
- Documentation of access termination upon employee departure
- Proof of breach notification compliance when incidents occur
The Compliance Audit Query Test
Your audit logging should answer these questions within minutes:
- Show all users who accessed patient [X]’s record in the last 90 days
- Show all patients whose records were accessed by user [Y] last month
- Show all emergency/break-glass access in the last quarter with post-access reviews.
- Show all access to substance abuse treatment records by users without documented authorization.
- Show all administrative users who accessed production PHI last week.
- Show all denied access attempts that might indicate unauthorized access attempts.
- Show all users who accessed more than 100 patient records in a single day.
- Show the complete access history for a specific encounter or clinical document.
If these queries take hours to run or require custom database queries, your audit infrastructure is inadequate. Compliance requires real-time or near-real-time answers.
Performance Considerations for Permission Evaluation
Complex authorization logic creates performance challenges. Every data access requires policy evaluation, relationship checking, and audit logging. Done naively, this adds 100-500ms of latency per request.
Optimization Strategies
Permission Caching with Invalidation: Cache authorization decisions for common access patterns. A physician viewing their own patient list shouldn’t re-evaluate care relationships on every page load. Cache these decisions with a short TTL (5-15 minutes) and invalidate when relationships change.
Batch Authorization: When displaying lists, batch evaluates permissions instead of checking each item individually. A single database query can verify care relationships for all patients in a list rather than N individual queries.
Materialized Views: Pre-compute common permission queries. Maintain materialized views of active care relationships, team memberships, and organizational hierarchies. Refresh periodically rather than computing on every request.
Policy Compilation: Compile high-level authorization policies into optimized query filters. Instead of evaluating complex rules in application code, generate WHERE clauses that push filtering to the database.
Layered Enforcement: Enforce coarse-grained permissions at the API gateway (organization access, basic role checking) and fine-grained permissions at the service layer. This prevents unauthorized requests from reaching expensive policy evaluation logic.
Implementation Roadmap
Building production-grade healthcare RBAC requires incremental implementation:
Phase 1: Foundation (Weeks 1-4)
- Define user roles and the initial permission matrix.
- Implement basic role checking at API boundaries.
- Establish audit logging infrastructure.
- Create patient-level data isolation.
Phase 2: Relationship-Based Access (Weeks 5-8)
- Model care relationships in the database
- Implement relationship-based authorization
- Add temporal constraints to access policies.
- Build a permission caching layer.
Phase 3: Fine-Grained Controls (Weeks 9-12)
- Implement field-level permissions
- Add data sensitivity classifications.
- Create operation-specific authorization
- Build break-glass access workflows.
Phase 4: Advanced Compliance (Weeks 13-16)
- Deploy anomaly detection on audit logs.
- Implement automated permission reviews.
- Create compliance reporting dashboards.
- Conduct security testing and penetration testing.
Phase 5: Optimization (Ongoing)
- Performance tuning of authorization queries
- Permission cache optimization
- Audit log storage optimization
- Continuous compliance monitoring
This timeline assumes dedicated engineering resources and clear requirements. Organizations with complex existing systems or regulatory requirements may need 6-9 months for complete implementation.
Partner with Trembit for Healthcare RBAC Architecture
Designing and implementing production-grade access control for healthcare platforms requires deep expertise in both technical architecture and regulatory compliance. Most development teams have built RBAC for standard SaaS applications. Very few have architected the multi-dimensional, audit-ready, compliance-focused access control that healthcare demands.
Trembit specializes in healthcare platform architecture with particular depth in role-based access control that withstands regulatory scrutiny. We understand the difference between “checking user roles” and “implementing attribute-based access control with relationship context, data sensitivity awareness, and comprehensive audit trails.”
We architect patient-level data isolation that prevents accidental exposure. We implement fine-grained permission layers that support complex clinical workflows. We build audit logging infrastructure that generates evidence that regulators actually accept. We design anomaly detection that identifies potential breaches before they become notification events.
When you need RBAC architecture that supports your clinical workflows, satisfies compliance requirements, and scales with your platform growth, we bring the expertise and engineering discipline to deliver it correctly the first time.